Multiple-bilateral-renal-calculi and medullary-nephrocalcinosis

medcases00
Published on Nov 10, 2021
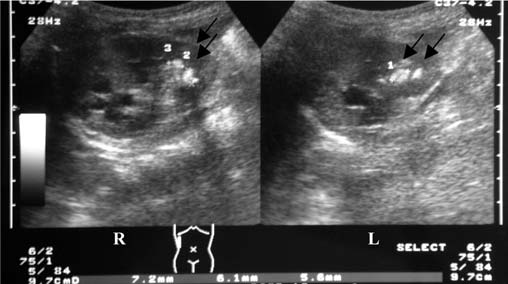
A 29-year-old woman with history of medullary sponge kidney treatment underwent SWL on bilateral nephrolithiasis. .2-mm and 8-mm stones were located in the right kidney (RK). In the left kidney (LK), there were 5-mm and 7-mm stones. One session of SWL was carried out in 75 min. 3600 shocks was delivered to RK and 2500 shocks was delivered to LK resulting in adequate stone fragmentation. The procedure was well tolerated, without any complications. One week later, the patient went to the hospital with a severe headache. Blood pressure at 200/110 mmHg was detected. She denies any previous history of sweating or flushing. Her BP was previously recorded as normal on PCP visit one year ago. no family history of HTN. Serum creatinine was normal range, K 4.5 range, Bicarb 22 . He was started on iv nicardipine drip for bp management without good response. She responded to iv vasotec for BP management. Next step in evaluating cause of her hypertension. She is not on any home medications prior to this admission. Her creatinine continues to remain normal 2 days later and her BP control improved.
A) Renal Doppler Ultrasound for RAS screening
B) Renal Ultrasound
C) check 24 urine for metanephrines
D) check plasma renin and aldosterone levels
E) CT angiogram to rule out fibromuscular dysplasia
SCROLL BELOW FOR ANSWER
Choice ( B) - Renal Ultrasound is the correct answer. This phenomenon results from external compression of the kidney by a subcapsular hematoma. It is a rare, treatable cause of secondary hypertension mediated by activation of the renin-angiotensin-aldosterone system (RAAS) and hence the ideal agents for the treatment of hypertension are RAAS blockers.Page kidney induced by SWL is a rare complication with an incidence rated around 0.5%. . Conservative treatment should be considered in clinically stable patients with use of antihypertensive agents . However, surgical evacuation is usually required in the event of persistent hypertension, a very large hematoma or decreased renal function. The two main goals of intervention are renal decompression by the evacuation of the hematoma by open or percutaneous drainage of the compressing collection. If the collection has been long-standing, a fibrocollagenous shell may have formed, and this may require decapsulation of this shell or even nephrectomy. Percutaneous drainage has been observed to have better success rates in subcapsular hematomas that are of less than three weeks duration. External compression of the kidney may be due to a collection of blood from Blunt trauma, Iatrogenic - following biopsy of native or transplant kidney, extracorporeal shockwave lithotripsy, ureteral surgery, sympathetic nerve block or Spontaneous - anticoagulation, AV malformation, tumor, vasculitis, pancreatitis. Non-bleeding causes of external compression include lymphoceles particularly around the transplanted kidney, urinoma, retroperitoneal paraganglioma, or large simple cysts. ultrasound (US) was performed in this patient and it showed subcapsular hematoma of 15.5 mm thickness in the RK.
Choice (A) is incorrect ( renal doppler) An acute rise in serum creatinine following the administration of angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) Should make one suspect hemodynamically significant RAS. In this case patient creatinine remains normal despite use of Enalapril.
Choice ( C) is incorrect - she has no clinical features of pheochromocytoma such as sweating, flushing. and is very rare condition
Choice (D) is incorrect - HTN is adrenal adenoma responds to RAAS blockade but she has normal potassium, no evidence of metabolic alkalosis making Primary adenoma less likely
Choice ( E) is incorrect - FMD should be suspected in a young woman below 3 years presenting with sudden Severe or resistant hypertension over a previously stable baseline with a significant increase in the serum creatinine concentration (≥0.5 to 1 mg/dL ) that occurs after the institution of therapy with an angiotensin-converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB) in the absence of an excessive reduction in blood pressure, An epigastric/abdominal bruit/flank pain are other features - In this patient creat remained stable and responded to iv vasotec.
Add to
Flag Case Quiz
Rate case quiz
Rate case quiz
Up next
Recommended
-
Watch Later
55-year-old male with post renal transplant with worsening renal function, HTN and gout attacks.
232 views 1420 days ago -
Watch Later
35 year old lady post renal transplant with diarrhea, weight loss and anasarca.
221 views 1672 days ago -
Watch Later
77-year-old man with a type 2 DM presents with worsening renal function and proteinuria
331 views 1503 days ago -
Watch Later
-
Watch Later
45 year old male with eye pain, blurred vision, renal insufficiency and proteinuria
314 views 1198 days ago -
Watch Later
22 year old lady with muscle weakness, renal insufficiency and proteinuria
318 views 1198 days ago -
Watch Later
![48-year-old man presents with acute onset right flank pain and nephrotic syndrome]()
48-year-old man presents with acute onset right flank pain and nephrotic syndrome
265 views 1607 days ago